
Quick Takeaways
- Three main tests - RPR (blood), rapid point‑of‑care, and PCR - differ in speed, cost, and accuracy.
- In the U.S., most private plans cover the RPR when ordered by a doctor; rapid tests often need a medical‑reason justification.
- In the UK, NHS covers RPR and PCR for symptomatic or high‑risk patients; private insurers follow similar rules.
- Know the CPT/HCPCS codes (e.g., 86403 for RPR) to avoid surprise bills.
- Use the checklist at the end to verify coverage before you get tested.
When a doctor suspects syphilis, the first question patients ask is, “Will my insurance pay for the test?” The answer depends on the test type, the reason it’s ordered, and the rules of the insurer. This guide walks you through every test option, explains how public and private payers treat them, and gives you a step‑by‑step plan to get the right test without a surprise bill.
Syphilis testing is a set of laboratory procedures that detect the bacterium Treponema pallidum or the antibodies it triggers in the body. The goal is to confirm infection early, guide treatment, and prevent transmission. Understanding the landscape of tests and insurance rules helps you stay in control of your health costs.
What Is Syphilis and Why Testing Matters
Syphilis is a sexually transmitted infection (STI) caused by the spirochete Treponema pallidum. If left untreated, it can progress through primary, secondary, latent, and tertiary stages, affecting the heart, brain, and other organs. Early detection through testing is the only reliable way to stop the disease before it causes serious damage.
The Centers for Disease Control and Prevention (CDC) recommends testing anyone with a new sexual partner, symptoms that suggest an STI, or a history of syphilis. In the UK, the National Health Service (NHS) follows similar guidance for high‑risk groups.
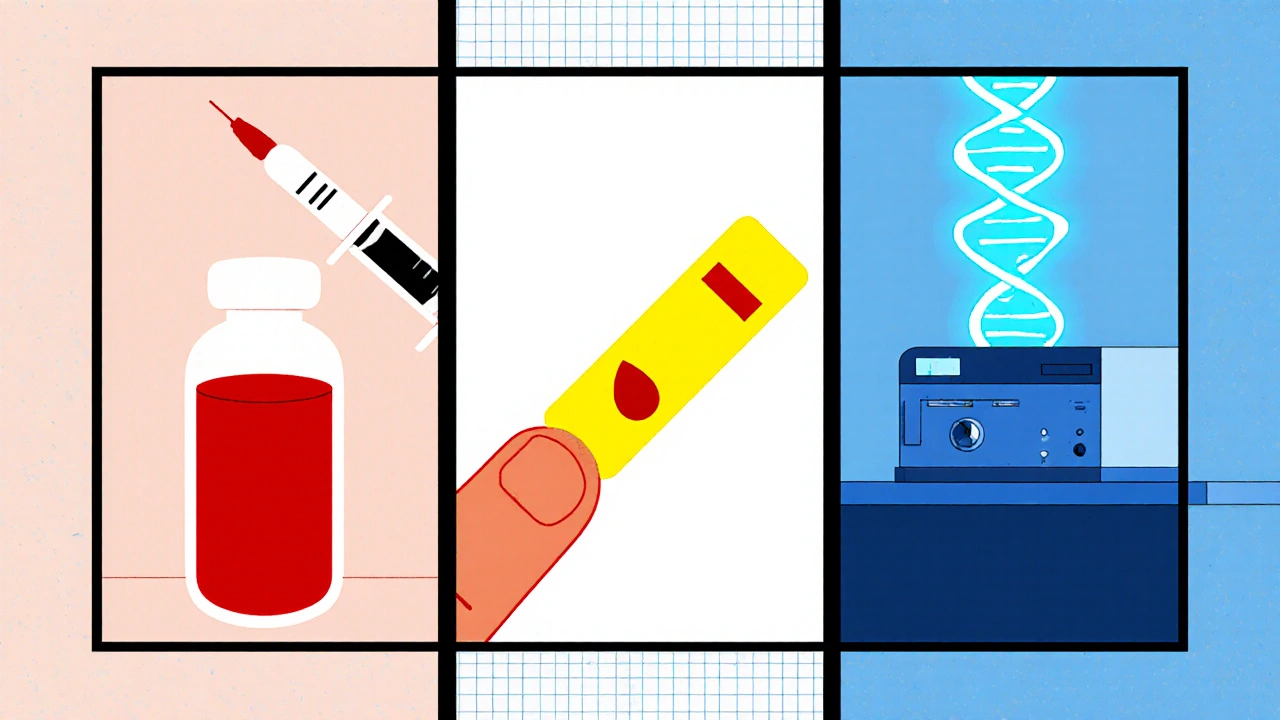
Types of Syphilis Tests
Three tests dominate clinical practice. Each has its own sample requirement, turnaround time, cost, and insurance friendliness.
| Test | Sample | Typical Turnaround | Average Cost (U.S.) | Accuracy |
|---|---|---|---|---|
| RPR (Rapid Plasma Reagin) | Venous blood | Same‑day or 1‑2 days | $30-$50 | 90‑95 % (screening) |
| Rapid point‑of‑care | Finger‑stick blood | 15 minutes | $60-$90 | 85‑90 % (screening) |
| PCR (Polymerase Chain Reaction) | Blood or lesion swab | 3‑5 days (lab) | $150-$250 | 98‑100 % (confirmatory) |
RPR (Rapid Plasma Reagin)
The RPR is the most common screening test. It looks for antibodies that the body makes in response to the infection. Because it’s inexpensive and widely available, most insurers consider it the standard of care for routine screening.
Rapid Point‑of‑Care Test
Designed for clinics that need results in minutes, the rapid test uses a finger‑stick sample. It’s convenient but slightly less accurate than RPR, so a positive result is usually confirmed with a laboratory test such as the TP‑PA (Treponema pallidum particle agglutination).
PCR (Polymerase Chain Reaction)
PCR directly detects the bacterial DNA. It’s the gold‑standard for confirming early infection or in cases where serology is ambiguous. Because it’s more expensive, insurers often require a documented medical necessity before covering it.
How Insurance Handles Coverage (U.S.)
Private health plans in the U.S. follow the CPT coding system. The most relevant codes are:
- 86403 - RPR test (screening)
- 86404 - RPR with reflex TP‑PA (confirmatory)
- 87591 - Rapid syphilis test (point‑of‑care)
- 87391 - PCR for T. pallidum
Most plans cover 86403 when a physician orders it for a patient with risk factors or symptoms. The rapid test (87591) often requires a “medical necessity” note because it’s considered a convenience test. PCR (87391) is usually covered only when the provider documents one of the following:
- Early primary lesions where serology may be negative.
- Pregnant patients with unclear serology.
- Research or public‑health investigations.
Medicaid and Medicare follow similar rules but differ by state. For example, California Medicaid (Medi-Cal) covers PCR for pregnant women, while Texas Medicaid does not.
How Insurance Handles Coverage (UK)
The NHS provides syphilis testing free of charge for anyone who meets the clinical criteria - typically symptomatic patients, pregnant women, or those identified as high risk through sexual health clinics. The NHS uses the same RPR and PCR assays as U.S. labs, so there’s no extra cost to the patient.
Private insurers in the UK (e.g., Bupa, Aviva) often mirror NHS policies. They will reimburse the RPR (CPT 86403) as an “essential health service” when a General Practitioner (GP) or specialist submits a claim with a diagnostic code (ICD‑10 A50‑A53). Rapid tests may be denied unless the GP notes a specific need, such as a community‑based outreach program.
Tips to Maximize Coverage
- Ask the clinician for the correct CPT code. A wrong code triggers automatic denial.
- Bring your insurance card and a written “medical necessity” note if you’re opting for a rapid or PCR test.
- Check your plan’s summary of benefits before the appointment. Look for language like “STI screening” or “preventive services”.
- If you’re uninsured, many public health departments offer free RPR testing. In the U.S., the CDC’s STD Testing Locator lists free clinics.
- In the UK, request a referral to a sexual health clinic (SHC) if your GP hesitates; SHCs are fully funded for STI testing.
Common Pitfalls and How to Avoid Them
Pitfall 1: Assuming “free” means fully covered. Some clinics bill a facility fee that your insurer may not see as a “lab test”. Ask for an itemized bill.
Pitfall 2: Ignoring prior‑authorization requirements. Certain insurers demand pre‑approval for PCR. Call the member services line before the appointment.
Pitfall 3: Mixing up codes. Using the code for “HIV test” (86701) instead of “Syphilis RPR” (86403) leads to claim rejections.
Checklist Before You Get Tested
- Verify your insurer’s coverage for RPR, rapid, and PCR tests.
- Confirm the clinician will order the test with the correct CPT/ICD code.
- Ask for a written medical‑necessity statement if you need a rapid or PCR test.
- Bring a copy of your insurance card and a note of any deductible.
- Know the expected out‑of‑pocket cost (most RPR tests are $0-$20 with insurance).
Frequently Asked Questions
Does Medicare cover syphilis testing?
Yes. Medicare Part B covers the RPR test (CPT 86403) when ordered by a physician for screening or diagnostic purposes. PCR is covered only for documented early infection or pregnancy‑related cases.
Can I get a syphilis test without a doctor’s order?
In many U.S. states you can purchase a home‑testing kit, but insurance won’t cover it. In the UK, you need a referral from a GP or can walk into a sexual health clinic, where the test is free.
What if my insurance denies the rapid test?
Request an appeal and submit the clinician’s medical‑necessity note. Most insurers will reconsider if you prove the test was needed for immediate treatment decisions.
How soon after exposure should I be tested?
RPR may be negative for up to 3 weeks after exposure. If you suspect recent exposure, ask for a PCR test, which can detect the bacteria within days.
Are there any free testing options?
Yes. In the U.S., CDC‑funded STD clinics and many community health centers provide free RPR testing. In the UK, all NHS sexual health clinics offer free testing for anyone who asks.
Knowing the right test, the correct code, and how your insurer works turns a potentially stressful medical visit into a smooth, cost‑predictable experience. Use the checklist, keep the FAQ handy, and don’t hesitate to ask your provider to clarify any coverage question before you roll up your sleeve.




Nathan Comstock
October 25, 2025 AT 12:08Listen up, folks – the American insurance system isn’t some hopeless mess when it comes to syphilis testing. The CPT code 86403 for the RPR is literally baked into private plans and Medicare, so you’re not left hanging. If a doctor orders it, the claim gets processed faster than you can say “preventive care.” Don’t let anyone tell you otherwise – we have the resources, we just need to use them.
Terell Moore
October 29, 2025 AT 19:34Ah, the classic American bravado – as if tossing around CPT codes somehow makes the whole system flawless. The guide pretends to be the ultimate authority while glossing over the labyrinthine prior‑auth hurdles that most patients never even hear about. Sure, the RPR is cheap, but try getting a PCR approved without a ten‑page justification and you’ll see the real cost. It’s all smoke and mirrors, really.
Amber Lintner
November 3, 2025 AT 04:01Really? That’s the angle you chose? Of course you can drum up the numbers and toss in some patriotic flair, but the real drama is in the patient who’s left waiting, sweating, wondering if that rapid test will ever get the green light. It’s not just about codes; it’s about people feeling abandoned by a system that pretends to be all‑knowing. And honestly, the guide could have used a little humility instead of shouting about superiority.
Lennox Anoff
November 7, 2025 AT 12:28Let me start by saying that the very existence of a guide like this highlights a societal failure to treat sexual health as a collective responsibility. In the United States, we pride ourselves on cutting‑edge diagnostics, yet we hide behind insurance bureaucracy that can delay life‑saving treatment. The United Kingdom, by contrast, provides universal coverage for syphilis testing through the NHS, reflecting a public health philosophy that places community well‑being above profit. This moral divergence is not merely academic; it has tangible consequences for individuals who cannot afford a $150 PCR test. Moreover, the guide mentions private insurers mirroring NHS policies, but they often lack the enforcement mechanisms that the NHS possesses, leading to inconsistent coverage. The moral imperative, therefore, is to advocate for policy reforms that eliminate prior‑authorization requirements for essential STI tests. One could argue that the CDC’s recommendation for universal screening is only as good as the infrastructure supporting it. When a patient is denied a rapid point‑of‑care test because of a “medical necessity” note, the system is effectively punishing transparency. The ethical question becomes: are we willing to accept another preventable infection spreading because of cost‑containment? In my view, the answer must be a resounding no. We need to shift the narrative from individual financial liability to collective health security. Furthermore, the guide’s focus on CPT codes, while useful, overlooks the broader context of health equity. A truly comprehensive approach would integrate social determinants of health, ensuring that marginalized populations receive the testing they need without financial barriers. In short, the guide is a step in the right direction, but it stops short of challenging the systemic inequities that make STI testing a privilege rather than a right. If we are to claim moral superiority, we must back it up with policies that guarantee access for all, regardless of socioeconomic status.
Olivia Harrison
November 11, 2025 AT 20:54Thanks for laying out all those points so clearly. I agree that making the testing process seamless and equitable should be a top priority. If clinicians help patients navigate the CPT codes and provide the necessary medical‑necessity documentation, many of those insurance hurdles can be avoided. Also, pushing for policy changes that eliminate prior‑auth for essential STI tests would benefit everyone. Let’s keep the conversation focused on actionable steps that help people get tested without surprise bills.
Bianca Larasati
November 16, 2025 AT 05:21You’ve got this-schedule that test and stay ahead of the game!
Corrine Johnson
November 20, 2025 AT 13:48Absolutely, darling; you’re absolutely right, of course, that a single sentence can inspire, motivate, and, let’s be honest, it also reminds us that sometimes less is more, especially when dealing with complex health topics, and, yes, keep that energy high, keep that spirit bright, keep pushing forward.
Jennifer Stubbs
November 24, 2025 AT 22:14From an analytical standpoint, the guide does a solid job summarizing CPT codes, but it glosses over the fact that Medicaid coverage varies dramatically by state, not just between California and Texas. Additionally, the discussion on prior‑authorization could benefit from concrete examples of how to appeal a denial. The omission of telehealth testing options, which have become more prevalent post‑COVID, is another gap. A more data‑driven section on cost‑comparisons across states would make the guide far more useful for readers navigating the patchwork of US insurance.
Abhinav B.
November 29, 2025 AT 06:41In India, sti testing is still shrouded in stigma, and many peope think it is a taboo topic – we have community health camps that offer free rpr tests, but insurance rarely covers anything unless it is part of a larger health package. The guide could have mentioned how cultural perceptions influence testing rates, becasue if you are afraid of being judged you will not even go for a test. Also, the cost of a pcr here is wildly different – it can be as high as 3000 rupees, which is a big barrier for many families.