Drug Interaction Type Checker
Check Interaction Type
Select two drugs to see their interaction type and explanation.
When you take more than one medication, something invisible is happening inside your body. Two drugs might seem harmless on their own, but together, they can cause serious side effects-or even cancel each other out. This isn’t random. It’s science. And it breaks down into two clear types: pharmacokinetic and pharmacodynamic drug interactions. Knowing the difference isn’t just for doctors. If you’re on five or more meds-especially if you’re over 65-this could save your life.
What Pharmacokinetic Interactions Do to Your Body
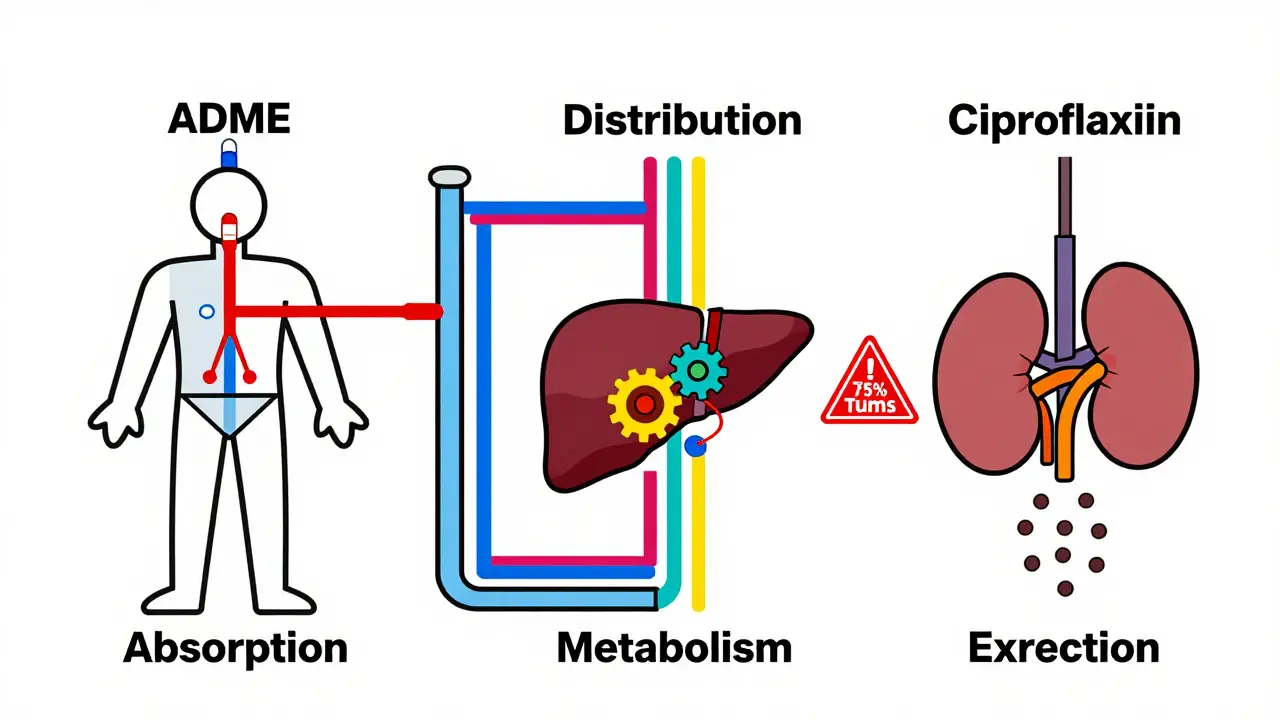
Pharmacokinetic interactions are about what your body does to the drug. Think of it like a delivery system. How fast does the drug get in? Where does it go? How long does it stay? And how does your body get rid of it? These are the four steps: absorption, distribution, metabolism, and excretion-or ADME for short.Let’s say you take an antibiotic like ciprofloxacin and an antacid like Tums at the same time. The antacid binds to the antibiotic in your stomach and stops it from being absorbed. Studies show this cuts absorption by 75% to 90%. The drug is still there. But your body never gets enough of it to work. That’s a pharmacokinetic interaction.
Another big player is metabolism. Most drugs are broken down by enzymes in your liver, especially a group called Cytochrome P450. The most common one is CYP3A4. It handles about 75% of all drug metabolism. Now imagine you’re taking simvastatin for cholesterol and start clarithromycin for an infection. Clarithromycin blocks CYP3A4. Suddenly, your body can’t break down simvastatin. Levels shoot up by 10 times. That’s not just a theory-it’s what happened in real patients. Some ended up with muscle damage so severe they needed hospital care.
Drug transporters matter too. Proteins like P-glycoprotein act like bouncers at the cell door. They push drugs out of cells or keep them from entering. If one drug blocks this transporter, another drug can pile up where it shouldn’t. This contributes to 15-20% of serious interactions.
These interactions are predictable. If you know which enzyme a drug uses, you can guess what will interfere. That’s why doctors check your meds before prescribing. They’re looking for red flags: antibiotics, antifungals, or heart meds that block CYP3A4, CYP2D6, or CYP2C9. The fix? Often, it’s simple: lower the dose, space out the pills, or switch to a different drug.
What Pharmacodynamic Interactions Do to Your Body
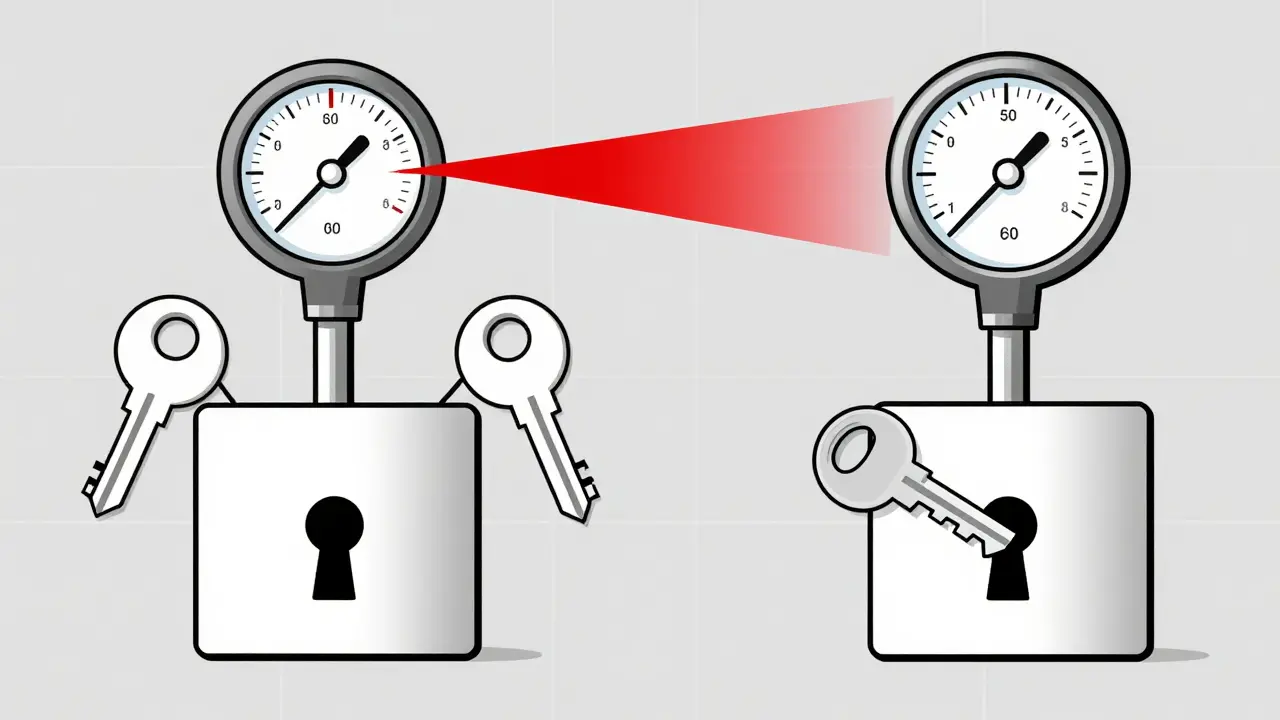
Now flip the script. Pharmacodynamic interactions aren’t about drug levels. They’re about what the drugs do when they meet at the receptor.Think of receptors like locks. Drugs are keys. If two keys fit the same lock, they can either turn it together, fight over it, or block it entirely.
Take sildenafil (Viagra) and nitroglycerin. Sildenafil relaxes blood vessels. Nitroglycerin does too. Together? Your blood pressure can crash. This isn’t because one drug increased the other’s level. It’s because both are hitting the same system-your blood vessels-with full force. That’s synergy. And it’s dangerous.
Another example: warfarin and aspirin. Warfarin thins blood by blocking vitamin K. Aspirin stops platelets from clumping. Neither changes the other’s concentration. But together, they double your bleeding risk. That’s additive.
Then there’s antagonism. Naloxone (Narcan) is the classic. It doesn’t reduce opioid levels. It just plugs the opioid receptors. No room for heroin or fentanyl to bind. The opioid can’t work. That’s why Narcan reverses overdoses so fast.
These are the sneakiest interactions. You won’t see a spike in drug levels on a blood test. You won’t know something’s wrong until you feel dizzy, pass out, or bleed internally. That’s why CNS drugs-antidepressants, antipsychotics, opioids-are high-risk. A 2023 review found that 85% of dangerous CNS interactions are pharmacodynamic. Serotonin syndrome from mixing SSRIs and MAO inhibitors? That’s PD. Opioid overdose? That’s PD. Even mixing NSAIDs with blood pressure meds like ACE inhibitors can make the BP drugs less effective by 25-30%.
The Key Difference: Concentration vs. Response
Here’s the simplest way to tell them apart:- Pharmacokinetic = How much drug is in your system.
- Pharmacodynamic = How your body responds to that drug.
Imagine a dose-response curve. PK interactions slide the curve left or right-changing the dose needed to get the same effect. PD interactions lift or lower the whole curve-changing how strong the effect can be, even at the same dose.
That’s why managing them is different. If a PK interaction happens, you can adjust the dose. Reduce simvastatin from 80mg to 10mg when taking clarithromycin. Monitor digoxin levels. Check INR for warfarin. Easy.
But if two drugs are fighting over the same receptor? No dose tweak helps. You have to avoid the combo entirely. That’s why the FDA and EMA list many PD interactions as absolute contraindications. No exceptions.
Who’s at Risk? And How Do We Catch These?
One in six adults over 65 takes five or more drugs daily. That’s 15% of older adults. And 6.7% of hospital admissions in the UK are due to drug interactions. Most are preventable.PK interactions are most common with drugs that have a narrow therapeutic index-tiny differences between a helpful dose and a toxic one. Think warfarin, digoxin, phenytoin, lithium. These need blood tests. Regularly.
PD interactions dominate in two areas: the brain and the heart. Antidepressants, opioids, blood pressure meds, and diabetes drugs are the usual suspects. You might not realize you’re at risk until you feel off. Fatigue. Confusion. Low blood pressure. Unexplained bruising.
Modern EHR systems now flag over 2,000 high-risk interactions. Epic’s 2023 update alone lists 1,247 PK and 983 PD interactions. But alerts aren’t perfect. Doctors get alert fatigue. Patients don’t always tell their pharmacist about supplements or OTC meds.
That’s where pharmacists come in. A 2022 survey found pharmacist-led medication reviews cut adverse events by 42%. They don’t just check for interactions. They ask: “What else are you taking?” Even that one herbal tea or pain reliever you don’t think matters.
What’s New? The Future of Drug Safety
The FDA now requires testing against 11 CYP enzymes and 8 transporters-not just 7. That’s a big jump. Why? Because we’re seeing more complex interactions than we used to.Pharmacogenomics is changing the game. Your genes affect how fast you metabolize drugs. If you’re a slow metabolizer of CYP2D6, even a small dose of codeine can turn into too much morphine. The CPIC now has 32 gene-drug pairs with clear guidelines. Testing isn’t routine yet-but it’s coming.
Real-world data is helping too. The FDA’s Sentinel Initiative found 17 new PD interactions in 2022. One? SGLT2 inhibitors (like Jardiance) with loop diuretics (like furosemide). Together, they increase dehydration risk by over 2 times. No one saw this coming from lab studies alone.
And now, AI is stepping in. A 2023 study in Nature Medicine trained a model to predict PD interactions with 89% accuracy. Traditional methods? Only 76%. That’s not science fiction. It’s already being tested in hospitals.
By 2030, better management of these interactions could prevent 1.3 million adverse events worldwide. That’s $28 billion in savings. Not just money. Lives.
What Should You Do?
If you take multiple medications:- Keep a written list. Include supplements, vitamins, and OTC drugs.
- Ask your pharmacist: “Could any of these interact?” Don’t wait for the doctor.
- Watch for new symptoms after starting a new drug. Dizziness? Nausea? Bleeding? Weakness? Tell someone.
- If you’re on warfarin, digoxin, or lithium-get your levels checked regularly.
- Never stop or change a dose without talking to your provider.
Pharmacokinetic and pharmacodynamic interactions aren’t abstract concepts. They’re real. They happen every day. And they’re often silent-until it’s too late. Understanding the difference gives you power. It lets you ask the right questions. And sometimes, that’s all it takes to stay safe.
Are pharmacokinetic interactions more dangerous than pharmacodynamic ones?
Not necessarily. PK interactions are more common and often easier to manage with dose changes or monitoring. But PD interactions can be deadlier because they’re harder to predict. For example, mixing two drugs that both lower blood pressure can cause sudden collapse-even if drug levels look normal. The danger depends on the drugs involved, not just the type of interaction.
Can over-the-counter drugs cause pharmacodynamic interactions?
Absolutely. NSAIDs like ibuprofen can reduce the effectiveness of blood pressure meds by blocking protective prostaglandins. Antihistamines like diphenhydramine (Benadryl) add to the sedative effects of opioids or antidepressants. Even herbal supplements like St. John’s Wort can interfere with serotonin levels. Many people assume OTC means safe-but that’s not true when combined with prescription drugs.
Why don’t blood tests always catch these interactions?
Blood tests only measure drug concentration. They don’t tell you what the drug is doing to your body. A pharmacodynamic interaction can happen even when drug levels are perfectly normal. For example, two drugs might both affect your heart rhythm independently. Together, they cause arrhythmia-even if neither drug level is too high. That’s why symptoms matter more than numbers sometimes.
Do all drug interactions show up right away?
No. PK interactions often take days to build up. For example, if a drug inhibits CYP3A4, it can take 3-5 days to reach full effect. PD interactions, however, can happen immediately. If you take a painkiller and a sedative together, you might feel dizzy within minutes. Timing matters-pay attention to when new symptoms appear after starting a new medication.
Can pharmacogenomics help prevent these interactions?
Yes. Your genes determine how fast you break down certain drugs. If you’re a slow metabolizer of CYP2C19, you’re at higher risk for bleeding with clopidogrel and PPIs. CPIC now has 32 gene-drug pairs with clear recommendations. Testing isn’t routine yet, but if you’re on multiple meds, especially for heart or mental health, ask if genetic testing could help.



jared baker
March 19, 2026 AT 07:03Just keep a list of everything you take-even gummy vitamins. I saw a guy on warfarin start taking turmeric for his knee and nearly bleed out. No one told him it was a problem. Simple fix: write it down. Talk to your pharmacist. Done.
Melissa Starks
March 20, 2026 AT 08:55I’m 72 and on 8 meds. I used to think if it wasn’t a prescription, it didn’t count. Then my doc caught that my daily ibuprofen was tanking my blood pressure med. I thought I was just being careful-turns out I was being dumb. Now I keep a little notebook. I even write down the herbal tea I drink. My pharmacist laughs but says I’m one of the few who actually listens. Don’t wait until you’re dizzy to start paying attention. Your body’s not playing games.
Michelle Jackson
March 21, 2026 AT 06:43Oh great, another ‘know your meds’ lecture. Like people actually read these things. I’ve seen 3 elderly folks in my building die from ‘interactions’-all had piles of pills but never asked a single question. It’s not the science that’s failing. It’s the people who think ‘it’s just Benadryl’ or ‘I’ve been taking this forever.’ Wake up. This isn’t rocket science. It’s basic responsibility.
Alexander Pitt
March 23, 2026 AT 05:19Pharmacodynamic interactions are the silent killers. You can have perfect lab numbers and still crash. I’ve seen it in the ER-two drugs, both normal levels, but together they trigger serotonin syndrome. No warning. No spike. Just sudden confusion, fever, tremors. If you’re on SSRIs and add anything-even tramadol or dextromethorphan-ask first. Always. This isn’t speculation. It’s documented. And it kills.
becca roberts
March 25, 2026 AT 03:42So let me get this straight-you’re telling me my chamomile tea and my Zoloft might be having a secret love affair in my brain? And I didn’t even know? I mean, I knew tea was ‘natural’ but I didn’t know natural meant ‘I’m about to hallucinate.’ Thanks for the heads up. Now I’m gonna go cry into my oat milk latte.
Andrew Muchmore
March 26, 2026 AT 06:39Don’t ignore the timing. PK interactions take days to build. PD can hit in minutes. If you start a new painkiller and feel dizzy 20 minutes later, don’t shrug it off. That’s not ‘just tired.’ That’s your brain telling you to stop. I’ve been there. Listen to your body before the ER listens to you.
David Robinson
March 26, 2026 AT 06:53Yeah but how many people actually do this? The system’s broken. Doctors are overworked. Pharmacies don’t have time. Patients don’t care. You can give me 1000 lists and 500 alerts, but if someone’s too lazy to read the damn label, you’re just shouting into the wind. This isn’t a knowledge problem. It’s a culture problem. We treat our bodies like disposable devices. And now we’re surprised when they break?
Paul Ratliff
March 27, 2026 AT 16:37My grandma took her blood pressure med and then a NyQuil. Passed out on the couch. They thought it was a stroke. Turned out it was the dextromethorphan + beta blocker combo. She’s fine now. But she’s also not taking NyQuil anymore. Simple. Why do we make this so complicated?
Melissa Stansbury
March 28, 2026 AT 11:53I’m a nurse. I’ve seen this too many times. A woman on lithium, started an OTC decongestant, and ended up in ICU with toxicity. She didn’t even know decongestants affected kidneys. We have to stop acting like patients are just ‘forgetful.’ They’re not given tools. No one shows them how to ask. No one says ‘this is why it matters.’ We need to stop assuming knowledge and start teaching context. A handout isn’t enough. You need to sit down. Ask. Listen. Then repeat. It’s not rocket science. It’s human.
Gaurav Kumar
March 29, 2026 AT 13:34Western medicine is so obsessed with reductionism. You break everything into enzymes and receptors. But life isn’t linear. Your body isn’t a machine. You can’t quantify human biology with CYP3A4 and P-glycoprotein. You need to look at the whole system-stress, sleep, gut health. These ‘interactions’ are symptoms of a broken lifestyle, not just bad drug combos. You want real safety? Fix your diet. Sleep. Breathe. Then worry about the pills.
Andrew Mamone
March 31, 2026 AT 00:14AI predicting PD interactions at 89% accuracy? That’s wild. I’ve been using a drug checker app for months now. It flagged a combo I didn’t even know existed-my antihistamine and my thyroid med. Turned out it was increasing my heart rate. I switched meds. No hospital visit. Just a phone app. Tech isn’t the enemy. Ignorance is. 🤖✅
SNEHA GUPTA
March 31, 2026 AT 01:17It’s funny how we treat drugs like they’re magical pills. We forget they’re chemicals. Real, physical, reactive molecules. Your body doesn’t care if it’s ‘prescribed’ or ‘natural.’ A molecule is a molecule. If it binds to a receptor, it’s going to do something. The idea that ‘herbal’ means ‘safe’ is dangerous. It’s not folklore. It’s pharmacology. And we’re all students here. No one knows everything. Not even doctors.
Suchi G.
March 31, 2026 AT 13:14I’ve been on antidepressants for 12 years. I started taking ashwagandha because I ‘needed to reduce stress.’ Then I got insomnia, heart palpitations, and a panic attack. My doctor said it was a PD interaction-ashwagandha boosts serotonin, and so does my SSRI. I thought it was ‘just herbs.’ I was wrong. Now I tell everyone: if it’s not on your pharmacy list, don’t add it. Your body doesn’t know the difference between ‘medicine’ and ‘supplement.’ It just reacts. And sometimes, it reacts hard.
Jeremy Van Veelen
April 2, 2026 AT 09:51Let’s be real-pharmacokinetic interactions are the easy ones. You adjust the dose. You monitor. You fix. But pharmacodynamic? That’s the dark magic. Two drugs, both perfectly legal, both prescribed, both ‘safe’… and together they turn your nervous system into a fireworks show. Serotonin syndrome. QT prolongation. Respiratory depression. No warning. No lab test. Just you, feeling like you’re dying, and no one knows why. That’s the real horror story. And it’s happening every single day.
Lauren Volpi
April 2, 2026 AT 14:04Wow. So we’re supposed to memorize enzyme names now? Next they’ll make us take a quiz before we can buy Advil. I’m just trying to live my life. I take my pills. I don’t need a PhD in pharmacology to survive. This post reads like a textbook written by someone who’s never met a real person.